The Pundit continues to have conversations with people who are sceptical that the COVID-19 outbreaks are a real health crisis.
These sceptics are driven by genuine concern about the enormous economic and social disruption occurring during this epidemic. The Pundit feels this "carnage" too.
It's good that they worry about this "shitstorm" as they call it.
But often it seems they don't have skills look hard and sceptically at the medical and biological damage, partly because evidence for this difficult to find. You need to search for reliable health indicators, and have biomedical research skills to find and interpret them.
Here are some findings from the Pundit looking at NSW Government health sources, supplemented with some most recent numbers from https://www.covid19data.com.au/, whom the Pundit admires and thanks.
First, how frequently are people dying from the Delta strain given they are infected?
This table shows a crude case fatality ratio based on counts of "local" infection in NSW.
These are almost exclusively caused by a single Delta variant strain of the virus.

As can be seen , local infection numbers took off explosively in July-August 2021.
One column in the table give the crude estimate of fatality rate (CFR) which is close to 1 death per 200 infections.
The problem with this raw death metric is that at the time deaths occurs, there are many detected infections in living people who will die at a later date and who don't get included in the metric. With infections doubling every week or so, about half the deaths will be missed.
The crude CFR measure is biased and is almost certainly an underestimate. We deserve to know the true value, but that's a time consuming bit of public health maths.
One way to (partly) correct for this bias is to use a different denominator in the ratio, that in effect gives more infected people time to die, and be included in the CFR fraction calculated. To do this, the Pundit used cumulative case numbers 14 days before the death count number in question, assuming severely sick people take on average two weeks to die. This metric is called CFR lag adjusted in the table.
This adjustment for indicates that death rates from COVID-19 are 10 per 1000 infections. Which is a pretty brutal statistic.
One encouraging possible trend shown in the table is the number of deaths per week which is relatively static for the last 4 entries in the time series. Possibly this indicates that immunisation programs are starting to mitigate the mortality impact of infection.
There are other brutal statistics to look at in the Sydney outbreak though:
In this table ratios, for hospital admissions and intensive care unit admissions analogous to the CFR mortality metric were also calculated and exhibited.
Hospital admissions are running at 150 new admissions a day per 1000 infected people, which is pretty sobering.
But it is the last ratio in the table, considered in combination with the CFR values that really jolted the Pundit.
Near 20 to 40 percent of people entering the ICU with COVID-19 are likely to die, and there are 20 to 30 ICU admissions per 1000 infections in Sydney.
That's a shitstorm that makes the Pundit really sad.
Post-Script
This topic was extensively discussed and its main points fully confirmed in several later posts
E.g.
Delta variant infections increase the risk of needing hospital care about two-fold.
29 08 2021 (Updated 4 September 2021)
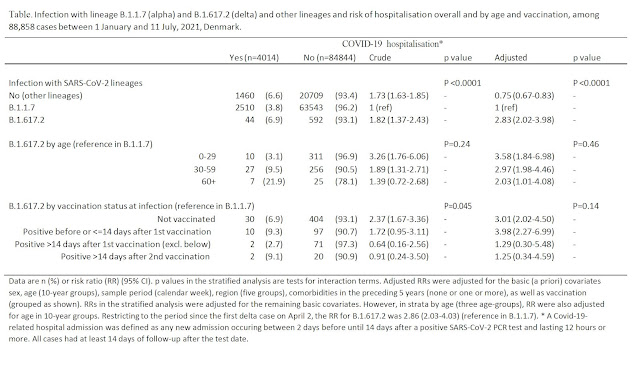
In the last few days a credible investigation of health risks from the Delta variant appeared in the medical journal Lancet infectious diseases (Twohig and colleagues). It suggest that there is increased risk of need hospitalisation with the Delta variant as compared to an earlier recognised alpha variant. It was followed a few days later by a study of infections in Denmark which found similar increases in risk of hospitalisation with the Delta variant (Bager and colleagues in Lancet Infectious diseses).
This table taken from the Lancet article compare the incidence of hospitalization per person stuient per unit of time tracked (hazard) for delta variant infections as compared to infections caused by an earlier variant .
They observe a 2-fold increased frequency for delta infections after adjusting for confounding factors like age of patients. Analogous 2-fold changes were seen by Bager and colleagues.
Hospital admission and emergency care attendance risk for
SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern:
a cohort study
Katherine A Twohig, MPH Tommy Nyberg, PhD Asad Zaidi, MSc Simon
Thelwall, PhD Mary A Sinnathamby, MPH Shirin Aliabadi, PhD et al.
The Lancet Infectious Diseases
August 27, 2021 DOI: https://doi.org/10.1016/S1473-3099(21)00475-8
Implications of all the available evidence
The evidence from these two studies in Scotland and England
consistently suggest that patients with COVID-19 who are infected with the
delta variant have approximately two times the risk of hospital admission
compared with patients with the alpha variant. These findings should be
considered for resource and policy planning in secondary care, particularly in
areas where the delta variant is increasing and is likely to become the
dominant circulating SARS-CoV-2 variant.
 |
| Supplement to Peter Bager; Jan Wohlfahrt; Morten Rasmussen; Mads Albertsen; Tyra Grove Krause 2021. |
1 October 2021Another article, Paredes and colleagues 2021 from a respected research group in Washington State makes the same point about Delta variant having more severe health impacts than ancestral strains of the SARS-CoV2 virus.
Here is a figure from this article:
In this table, the hazard ratio is an adjusted ratio of risk measure for hospitalisation events in individuals from Washington State who are diagnosed with COVID-19 caused by different virus variants. Each variant was characterised by molecular characterisation of virus genes. It confirms that Delta variant infected people are about 2-fold more likely to seek hospital care than similar people infected with the early variant of the virus.
Preprint Associations between SARS-CoV-2 variants and risk of
COVID-19 hospitalization among confirmed cases in Washington State: a retrospective
cohort study
Interpretation: Infection with a Variant of Concern [including
Delta] results in a higher hospitalization risk, with an active vaccination attenuating
that risk. Our findings support promoting hospital preparedness, vaccination,
and robust genomic surveillance.
Miguel I. Paredes* , Stephanie M. Lunn, Michael Famulare , and
others
https://www.medrxiv.org/content/10.1101/2021.09.29.21264272v1.full.pdf
Is Delta worse for children?
Eric Topol on Twitter just tweeted about Delta variant in US Children
He mentions:
Here's a key graph from that study:
Note the relative increase in 5 to 11 year olds during the Delta wave. Other findings in the paper show that low vaccination rates lead to higher incidence in children during the 2021 US Delta variant wave of disease.
See also
Delahoy MJ, Ujamaa D, Whitaker M, et al. Hospitalizations Associated with COVID-19 Among Children and Adolescents — COVID-NET, 14 States, March 1, 2020–August 14, 2021. MMWR Morb Mortal Wkly Rep. ePub: 3 September 2021. DOI:
http://dx.doi.org/10.15585/mmwr.mm7036e2









This comment has been removed by a blog administrator.
ReplyDelete